


Quality assurance in behavioral health billing catches errors at every stage, front desk intake, documentation, coding, and authorization, before they trigger claim denials. By building standardized checkpoints, automated eligibility alerts, and pre-submission review processes into your daily workflow, you’ll flag coverage lapses, coding-documentation mismatches, and incomplete data before claims ever reach the payer. This shifts your billing operation from reactive denial management to preventive compliance. Below, you’ll find the specific workflows that make it work.
Why Behavioral Health Claims Face Higher Denial Rates

Behavioral health claims deny at considerably higher rates than medical or surgical claims, not because behavioral health billing is inherently more difficult, but because payers impose layered requirements that create more points of failure. You’re maneuvering through stricter prior authorization demands, ongoing utilization reviews, payer-specific documentation language, and narrow coding requirements simultaneously. Each layer introduces distinct denial risk. The reality is that most denials are preventable and follow identifiable patterns, making systematic quality checks essential before claims ever reach the payer.
Without quality assurance in behavioral health billing, these compounding vulnerabilities go unchecked. A lapsed authorization, a missing modifier, an uncredentialed provider, or a progress note lacking functional impairment language, any single gap triggers a denial. Payers now deploy AI-driven claim analysis that flags deficiencies automatically, meaning errors you’d previously resolve informally now generate immediate denials at scale.
Catch Behavioral Health Billing Errors at the Front Desk
Before a claim ever reaches the billing team, the front desk has already determined whether it will pay or deny. Patient name misspellings, incorrect dates of birth, and wrong insurance IDs trigger immediate rejections, errors that no downstream QA billing process can efficiently recover.
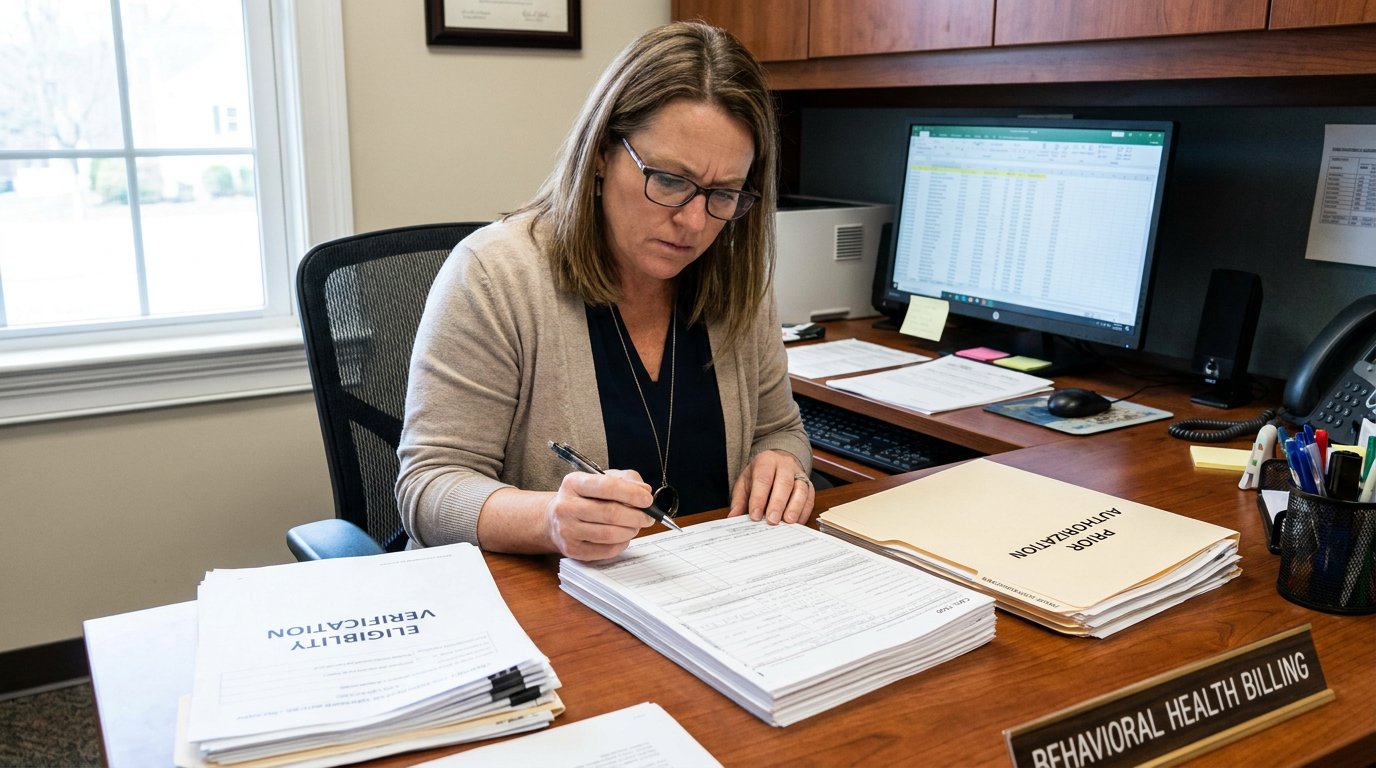
You’ll prevent these denials by standardizing your front desk workflow with structured intake checklists. Verify insurance eligibility before every service period using real-time verification tools. Confirm prior authorization requirements and session limits upfront. In behavioral health, where payer rules shift frequently, automated eligibility checks and expiration alerts aren’t optional, they’re essential. Failing to identify behavioral health carve-outs to Managed Behavioral Health Organizations can result in denied claims mid-treatment, even when coverage initially appears active.
Assign dedicated staff to verification, and maintain open communication between clinical and front desk teams so documentation aligns with billing from the start.
Write Documentation That Justifies Every Code You Bill
When a payer audits a behavioral health claim, the documentation is the only evidence that the service occurred as billed, and if the note doesn’t support the code, the revenue gets recouped regardless of what actually happened in the session. Billing accuracy behavioral health depends on notes that directly align with CPT requirements. Best practices for claim submission include ensuring that all documentation is complete and accurate. Clear and thorough notes can significantly reduce the likelihood of audits and payment delays.
Every note must include:
- Exact start and stop times for time-based codes, 53+ documented minutes for 90837, not “approximately one hour”
- Named interventions and patient response, “CBT targeting avoidance behaviors” rather than generic “therapy provided”
- Medical necessity linkage connecting the primary diagnosis, functional impairment, and treatment goals to the specific service billed
For diagnostic evaluations billed under 90791 or 90792, documentation must include history, mental status exam, risk assessment, diagnosis, and treatment plan, and clinicians should note that these codes cannot be billed alongside a full psychotherapy session on the same day.
You can’t bill what you can’t prove. Structure your documentation to withstand audit scrutiny before submission.
Align Your Coding to Prevent Denials Before Submission
Your coding alignment process must verify that every CPT and ICD-10 code pair directly corresponds to what’s documented in the clinical record, because payers will deny claims where the diagnosis doesn’t support the procedure billed. You should build pre-submission checks that confirm code-to-documentation accuracy, flag mismatches between authorization details and selected codes, and catch modifier errors before claims leave your system. Beyond internal alignment, you need to actively track payer-specific coding updates and policy changes so your team isn’t billing against outdated rules that guarantee preventable denials.
Match Codes With Documentation
Every claim denial traced back to a coding-documentation mismatch represents a preventable failure, one that a structured pre-submission claim review process eliminates. Your documentation must directly substantiate every code on the claim, no exceptions.
Before submission, verify these critical alignment points:
- Time documentation matches CPT thresholds exactly, confirm recorded start and end times support the billed code, particularly for 90832, 90834, and 90837, where minute ranges determine code eligibility.
- ICD-10 diagnosis pointers link correctly to each CPT code, use specific F-codes rather than generic Z-codes to establish medical necessity.
- Provider credentials authorize the billed service, confirm scope-of-practice restrictions don’t invalidate the claim, such as LMSW limitations on diagnostic evaluations.
Each checkpoint closes a specific denial pathway before the claim leaves your system.
Track Payer Coding Updates
Payer coding rules shift multiple times per year, and each update creates new denial exposure if your billing team doesn’t catch it before submission. Monitor CMS HCPCS Quarterly Updates, AMA CPT changes, and individual payer policy bulletins on a fixed schedule. Pay close attention to modifier 25 reimbursement changes, automatic downcoding rules, and prepayment edits expanding across E/M levels 4 and 5.
Assign a specific team member to track payer-specific coding revisions and flag policy shifts that affect behavioral health services. Use real-time EHR edits and claims scrubbing tools to apply updated rules before claims leave your system. This structured approach to error prevention behavioral health claims keeps your coding aligned with current payer expectations and eliminates preventable denials at the source.
Build a Behavioral Health QA Workflow That Flags Gaps

You can’t catch billing gaps consistently through manual review alone, you need automated eligibility alerts that flag coverage lapses, authorization expirations, and enrollment changes before claims reach submission. Pair those alerts with standardized chart review checkpoints that require verification of documentation completeness, coding accuracy, and authorization validity at defined intervals before any claim generates. When you build these two mechanisms into your daily workflow, you create a systematic barrier between incomplete claims and payer submission that reduces denial exposure and audit risk.
Automate Eligibility Gap Alerts
When eligibility gaps slip past your front-end checks, they don’t surface again until a payer returns a denial, at which point you’ve already delivered the service, consumed clinical resources, and lost the window to collect from the patient or secure alternative coverage. Automated eligibility gap alerts eliminate this exposure by flagging coverage issues before claims enter your submission queue.
Effective behavioral health billing quality control requires structured exception routing: The importance of billing metrics in healthcare cannot be overstated. These metrics provide insights into financial performance, helping organizations identify areas for improvement.
- Active coverage with incomplete data routes to staff for verification completion, preventing downstream denials from missing benefit details.
- Terminated coverage triggers automated member outreach and insurance discovery workflows to identify alternative payers.
- Authorization requirements flag automatically based on scheduled procedure codes and payer contract configurations.
Practices using defined exception workflows reduce manual follow-up time by 65%.
Standardize Chart Review Checkpoints
Even if your eligibility checks and authorization workflows run flawlessly, claims still fail when the underlying clinical documentation doesn’t support the services billed, which is why standardized chart review checkpoints serve as your last line of defense before submission. Every chart should pass through a defined verification sequence: DSM-5 diagnosis with documented criteria linkage, measurable treatment plan goals aligned to interventions, signed progress notes with matching procedure codes, and completed risk assessments including MSE and SI/HI screening.
For effective claim error prevention behavioral health teams should adopt a CQRT-style monthly review covering at least 5% of eligible charts. Select charts strategically, random samples, high-risk cases, and previously denied claims. Score each consistently as compliant, needs improvement, or non-compliant, then route deficiencies for correction before submission.
Track Denial Trends to Improve Billing Outcomes
Because denial patterns reveal systemic weaknesses in your billing workflow, tracking them isn’t optional, it’s a compliance and revenue protection requirement. You need centralized denial logging that captures payer, denial code, dollar amount, and root cause in a single source of truth. Without this, your billing QA workflow in behavioral health operates reactively instead of preventively. Inhouse billing efficiency strategies play a crucial role in minimizing denials and maximizing revenue. By implementing these strategies, organizations can enhance their workflows and ensure timely processing of claims.
Denial tracking isn’t optional, it’s how your billing QA shifts from reactive cleanup to preventive compliance protection.
Monthly trend analysis should drive your corrective actions:
- Monitor denial rates against industry benchmarks (6, 13%) to identify when your facility exceeds acceptable thresholds
- Conduct root cause analysis on your top five denial reasons to isolate coding, authorization, or documentation failures
- Use predictive analytics to flag high-risk claims before submission, reducing rework costs and accelerating cash flow
Call Now and Simplify Your Billing Process
Revenue challenges should never distract you from the work that matters most. At Arise Billing Solutions, our experienced U.S.-based team manages your entire billing cycle with accuracy, transparency, and integrity. Call +1 (747) 256-6600 today and let us help you take control of your revenue.
Frequently Asked Questions
How Often Should Behavioral Health Billing QA Audits Be Conducted?
You should conduct QA audits at least quarterly to detect errors early and maintain compliance. If you’re running a high-volume practice or processing complex claims, you’ll want to move to monthly audits to catch recurring mistakes promptly. Regardless of your practice size, you must perform a thorough annual audit to assess overall compliance and uncover long-term trends. Consistent scheduling reduces denial rates by 20, 40% and prepares you for payer scrutiny.
What Software Tools Best Support Quality Assurance in Behavioral Health Billing?
You’ll find the strongest QA support in platforms that automate pre-submission checks. Passage Health flags payor-specific violations and links sessions to correct billing codes automatically. CentralReach offers rule-based claims editing across multi-location organizations. Qualifacts builds eligibility verification and claims editing directly into the workflow. TheraNest and TherapyNotes catch errors in real time with integrated documentation checks. Prioritize tools that enforce compliance rules before claims ever reach the payor.
Who Should Be Responsible for Overseeing the QA Process Daily?
You should assign daily QA oversight to a dedicated Quality Management Program Coordinator who chairs your Quality Improvement Committee. This person drives accountability across billing, compliance, and clinical documentation teams. You’ll also want internal audit staff performing real-time checks within the billing cycle, catching discrepancies before submission. Cross-functional committee involvement from credentialing, medical records, and compliance guarantees no single department bears sole responsibility, distributing risk and strengthening your overall process controls.
How Does Outsourcing Billing Affect Internal Quality Assurance Effectiveness?
Outsourcing billing can strengthen your QA effectiveness if you select a HIPAA-compliant partner with defined KPIs, but it introduces risks you must actively manage. You’ll gain specialized expertise and higher clean claim rates, typically 10, 20% improvement, while reducing overhead. However, you’re also accepting potential gaps in communication, privacy exposure, and diminished direct control. You’ll need continuous compliance monitoring, clear performance benchmarks, and regular audits to maintain accountability.
What Training Do Billing Staff Need to Perform Effective QA Reviews?
You need to train your billing staff in specialty-specific coding guidelines, modifier usage, bundling rules, and payer-specific edit requirements. They’ll also need proficiency in documentation review, medical necessity validation, and authorization verification. Include denial root-cause analysis training so reviewers recognize high-risk claim patterns. Implement risk-based sampling protocols and checklist-driven workflows to standardize reviews. When you identify defects, deliver targeted refresher training within seven days to close knowledge gaps quickly.